

What is a Hernia?
A hernia is a bulge or lump that occurs when there is a weakness in the muscles or tissue of the abdomen wall. This weakness allows some of the contents of the abdomen to push through the weakened area inside a sac to be outside the muscle wall but below the skin. Most hernia only contain fatty tissue, but as they enlarge some will contain bowel or intestine.
There are many different types of hernia. The most common is the inguinal hernia which occurs in the groin area and predominantly in men. Other hernias can occur in the navel (umbilical hernia), under the groin ligaments (femoral hernia), under large incisions (incisional hernia), and through the diaphragm into the chest (hiatus hernia).
As a rule, sufferers first become aware of a hernia when they notice a lump or a swelling or notice pain in the affected area. Hernias are usually more obvious to the eye when standing, coughing or straining. Most hernias will reduce back inside the muscle wall when the sufferer lies down. If the hernia does not ‘disappear’ when the patient is lying down, it may be ‘incarcerated’ or ‘strangulated’ and need urgent assessment for surgery.
Who is at risk?
A hernia can develop in anyone, from a newborn baby to a senior citizen. The following factors can increase an individual’s risk to suffering a hernia by straining or increasing pressure on the abdominal wall:
Obesity
Straining during bowel movements
Pregnancy
Straining to lift heavy objects
A chronic cough such as a smoker’s cough
Persistent sneezing caused by an allergy
Inguinal Hernia
An inguinal hernia is the most common type of hernia. About 9 out of 10 Hernias are inguinal. They are mostly found in males but can also occur in women.
They are caused by a weakness or a stretching of the muscles of the inguinal (groin) area. These muscles normally hold the organs and surrounding tissues in place. An organ such as the Intestine can push the abdominal lining through the weakness and form a balloon-like sac just below the skin.
Over time, an untreated hernia will continue to push, enlarging and protruding down to the pubic area and in men into the scrotum.
The inguinal canal is the path of the descent of the testis to the scrotum and remains a natural weak point in the abdominal muscles in men. This is aggravated by injury or repeated strain of the abdominal muscles such as chronic cough, constipation or heavy lifting, and often causes significant pain, which usually gets worse with time.
Hernia repair is one of the most commonly performed operations. Special belts can be used to support the hernia, but the best treatment is surgery.

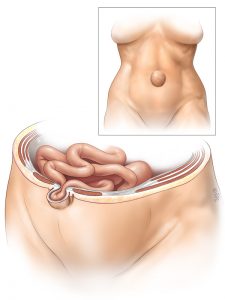
Umbilical Hernia
An umbilical hernia is a protrusion of the abdominal lining, or a portion of abdominal organ(s), through the area around the navel (belly-button). This can be an area of natural weakness in the abdomen as the umbilicus is made up of tissue that is thinner than the rest of the abdomen.
Depending on the severity of the hernia, the area of the defect can vary in size, from less than 1 to more than 5 centimeters in diameter.
In rare cases, bowel or other tissue can protrude and become strangulated through the lack of blood flow to a section of bowel. This would require emergency surgery.
Femoral Hernia
A femoral hernia occurs when there is a weakness in the tissues under the main groin ligament and is next to the point where the blood vessels and nerves pass from the abdomen into the leg. More common in females because it appears that pregnancy may weaken the abdominal tissues. Sufferers will sometimes become aware of a small swelling close to the pubic bone in the groin.If the hernia contains bowel there is a high chance of the bowel twisting or obstructing, causing a bowel obstruction.
A femoral hernia can cause serious medical problems if left untreated, even if there are no troublesome symptoms to begin with. Treatment is by an operation to return the herniated intestine to its proper place and close the weakness in the abdominal wall.

Epigastric Hernia
A epigastric hernia is composed usually of fatty tissue and rarely contain intestine. Formed in an area of relative weakness, gap or opening betweem the muscles of the abdominal wall.
They appear on a line between the breast bone and the navel or umbilicus and results in a bulge of intra-abdominal contents and/or pain or discomfort. This pain and discomfort is the result of nerves and tissue in this area being irritated or stretched as the surrounding tissue is also stretched.
If these hernias enlarge, intestine may become trapped within the hernia leading to intestinal blockage or damage through strangulation or incarceration. This is considered a surgical emergency.
Men are about three times more likely to have an epigastric hernia than women, and the majority occur in people aged between 20 years of age and 50 years of age. This hernia type is easily repaired and usually as a day case.

Hiatus Hernia
A hiatus hernia is due to a weakness of the diaphragm muscle which allows the stomach to herniate back into the chest. This commonly causes symptoms such as heartburn, nausea and can sometimes cause difficulty with swallowing. This occurs because the formation of the hernia often interferes with the barrier (lower oesophageal sphincter) which prevents acid from refluxing from the stomach into the oesophagus.
In individuals with hiatal hernias, the opening of the oesophageal hiatus (hiatal opening) is larger than normal, and a portion of the upper stomach slips up or passes (herniates) through the hiatus and into the chest.
Other factors contributing to the development of such a hernia include: A permanent shortening of the oesophagus (perhaps caused by inflammation and scarring from the reflux or regurgitation of stomach acid) which pulls the stomach up; and an abnormally loose attachment of the esophagus to the diaphragm which allows the esophagus and stomach to slip upwards. They are more common in overweight people.
